An overburdened system

Ever since he was a kid, Josh Lewis dreamed of being a sportswriter.
He grew up in Crapaud, a tiny hamlet on the south shore of PEI, between Charlottetown and the Confederation Bridge.
Although he decided to take political studies at the University of Prince Edward Island, he hung on to his journalism dreams, doing written and broadcast work on the side.
Once he graduated in 2008, he decided to try the field full time, and snagged a job with a group of small weekly papers in Kindersley, Saskatchewan.
Within three years, Lewis had moved up to the larger Estevan Mercury.
His career seemed well on its way.
But then the depression set in.
Daily tasks became harder as his energy level dropped; he withdrew socially, and even interviewing people he knew well made him anxious.
“During that stretch I would get these crippling bouts of up to a week at a time; I really did just stop functioning,” he said while sipping on an iced tea at a Charlottetown Tim Hortons. “It sort of affected every aspect of my job.”
He knew he needed help, and in Saskatchewan he got it.
“Within two weeks of calling the mental health line, I had a therapist…. So that was great, and I could see her as often as I needed to.”
Eventually, Lewis’s employer told him about an insurance program at work that would allow him to take some time off. He came back to the Island in February 2015, and stayed.
He was in for a shock about PEI’s mental health system.
It took seven months to get an appointment with a psychologist, and seeing a psychiatrist took even longer.
“My family doctor referred me to different psychiatrists, and I never heard back from them, and honestly, I only got (a) psychiatrist by going to emergency,” he said.

caption
The Charlottetown emergency department where Josh Lewis sought help.That was just after Christmas 2016, almost two years after the first referral.
Desperate for help, he exaggerated his symptoms.
“I was sitting for five or six hours because it was a low priority case, and I was definitely conscious of that and thinking ‘how do I want to frame this?’ to make sure that I get some help.”
The big shift
At one time, governments across Canada treated the mentally ill by putting them in asylums that kept them out of sight and out of mind. That’s in the past now, but the community-based mental health system that has evolved in the wake of “deinstitutionalization” has problems of its own, and in areas away from major population centres, it can be even tougher to get care.
An investigation by journalism students at the University of King’s College has found that despite spending more than $200 million a year in Nova Scotia, and $33 million in PEI, an over-stressed mental health system is failing to provide prompt, effective care to many residents of Nova Scotia and Prince Edward Island.
There are shortages of family doctors, psychiatrists and other professionals who are key to good care, a scattered supply of acute psychiatric beds in hospitals, and gaps in services.
On the ground, patients and patient advocates interviewed by King’s students say getting the care they need is often a struggle, and once they get it, it can fall short.
Publicly reported waiting times for mental health services have recently reached as long as a year in Cape Breton, and far exceed official targets in many other areas of Nova Scotia and PEI. Figures obtained through a freedom of information request show in extreme cases, waits can stretch into years.
Residents, sometimes lacking other ways of accessing the care they need, show up in crisis at hospital emergency departments that are ill suited for the purpose.
“I think there’s expert medical care, nursing care, which certainly works very well in the larger urban settings,” said Dr. Michael Teehan, now head and clinical chief of Dalhousie University’s psychiatry department and a former head of the Canadian Psychiatric Association.
“It’s much more difficult in rural settings to access that kind of care, although the people who are practicing are as well-trained as anybody in the city. They’re just stretched beyond capacity.”

caption
Dr. Michael TeehanSome advocates and critics call it a crisis. Those running the system say not only is there no crisis, but that calling it that could undermine public confidence and dissuade people from seeking care.
$50 billion annual burden
The impact of mental health on Canadian society is staggering, affecting an estimated one in five Canadians and costing the economy at least $50 billion a year, or $1.2 billion annually in Nova Scotia and PEI, according to estimates prepared for the Mental Health Commission of Canada.
When family members are considered, almost everyone is affected.
According to data on hospital stays for which the discharge was in 2014, provided to King’s students by the Canadian Institute for Health Information, the amount of time spent in hospital for mental health disorders was the equivalent of taking 340 people out of Nova Scotia society, for a full year each. In PEI, it was the equivalent of 66 people for a year each.
The math is sobering, yet less than a tenth of the health budget in either province is spent on mental health, about 225 dollars per resident, in each province, on hospital and community services and physician billings (there are also related expenditures, such as pharmacare payments for mental health drugs). The recent money committed in health accords with the two provinces will increase that marginally, by close to $15 per person.
The challenge
The mental health systems of the two provinces have to deal with a wide range of ailments, from people encountering mild depression or anxiety for the first time, to those affected for a lifetime by severe disorders. Most illnesses are mild, but the worst can require long-term or intermittent hospitalization and years of therapy. People may get help from their family doctor, if they have one, from psychiatrists, community-based programs, or in hospitals.
The challenge for the system, and for patients, is that while many people get good care and are able to function much as before, the resources are stretched and waiting times can become longer and longer, especially in areas away from the regional centre of Halifax.
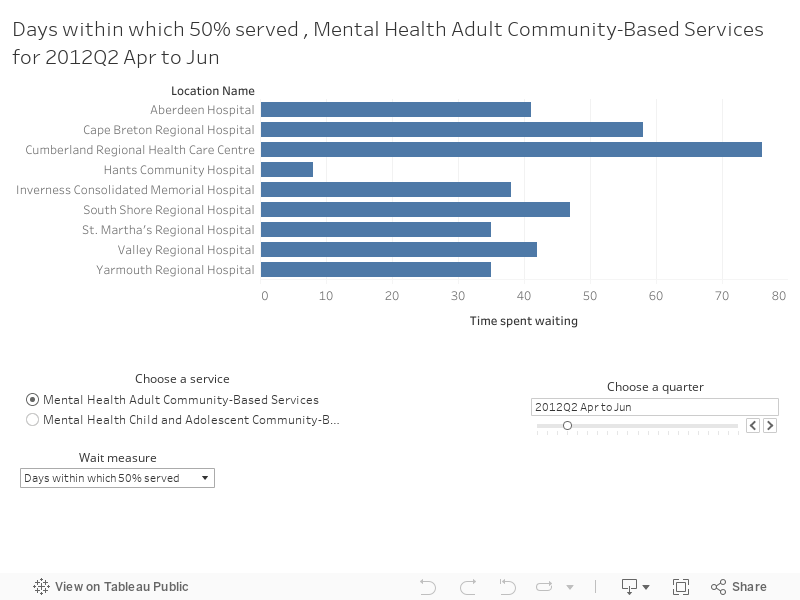
Interactive feature: see how long people waited for mental health services in Nova Scotia. Choose the quarter, type of service, and the wait time measure.
If you are using a small mobile device, this is best viewed by flipping your device to horizontal orientation.
Long waits
Colleen D’Orsay was diagnosed with depression when she was 19.
About three years ago the mother of three from Sydney ended up in a crisis at the emergency department at the Cape Breton Regional Hospital. Enrolled in a Master of Counselling Psychology program with New Brunswick’s Yorkville University, the last thing she wanted was a hospital stay.
“That was the only thing that I had, that I really felt good and proud of in my life. So if I had lost that, that would have made my health deteriorate even further.”
So the next morning, D’Orsay made an agreement with the psychiatrist on duty at the hospital. She wouldn’t be admitted, but she’d see a psychiatrist within two weeks.
“Almost a year to the date later, I got that phone call,” she said.
“So I waited in acute crisis for a year, when I was supposed to be getting that call within two weeks.”
D’Orsay’s experience might seem extreme, but official numbers published by the Nova Scotia Department of Health and Wellness show waits of that length are not uncommon for adult community based mental health services.
Waits are at some of the longest they’ve been since 2012 at some hospitals and clinics in Nova Scotia.
At the Cape Breton Regional Hospital where D’Orsay was treated, it took 354 days, almost a year, to serve 90 per cent of those waiting for adult mental health services, as measured in the last three months of 2016. A King’s Journalism analysis of the numbers shows as the wait times have increased, the number of patients treated there has fallen. The longest individual waits at Cape Breton Regional have been two years or longer, according to additional data released by the Nova Scotia Health Authority.
The queues for treatment are so long, that Cape Breton folk musician Rob Murphy was inspired to write a song about it.
“And it’s been 300 days since she asked for help,” he sings in the video posted on YouTube. “The voices in her head took away her life.”
“It’s been overwhelming, to say the least,” said Murphy of the thousands of messages he’s received since posting the video, “people that went and they sat at the hospital and they’ve been told ‘you can see a psychiatrist, but you have to get you doctor’s referral, and it’s a year wait…’
They just need somebody to talk to.”
The senior director of mental health and addictions with the Nova Scotia Health Authority, Linda Courey, calls these wait times “unacceptably long,” though she notes some rural areas such as that served by the Inverness Hospital have much shorter waits.
The health authority was created in 2015 and amalgamated nine district health authorities across Nova Scotia.
Courey said not only did the different authorities have different approaches to how people were assessed and put on waiting lists, approaches that have to be harmonized, but the system has to be restructured so people are getting the right care from the right professionals. The authority is working on a long-range plan to improve how mental health care is delivered in the province, which will be phased in over five to 10 years.
See how long people waited in PEI.
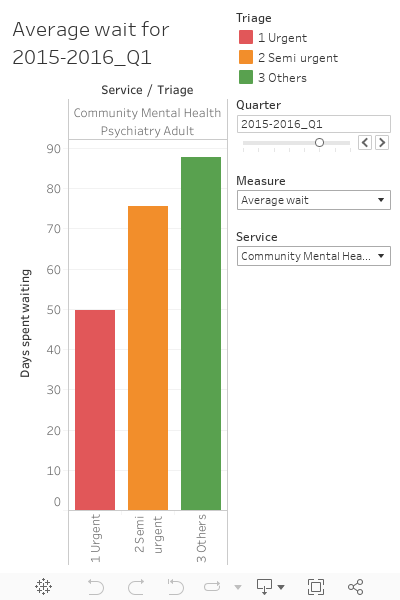
In Prince Edward Island, where Josh Lewis spent two years desperately hoping to see a psychiatrist, there are also long waits. The province is missing almost all of its targets for mental health wait times. In the last three months of 2015, the last period for which numbers are available, it took more than 16 months for 90 per cent of adults triaged as urgently needing to see a psychiatrist to be seen, and about 10 months for those triaged as semi-urgent, according to figures released by Health PEI. Waits for youth triaged as urgent were a bit shorter, with 90 per cent seen within three and a half months, while it took between 40 days and nearly 10 months for 90 per cent of those waiting for community-based mental health services to be seen, depending on urgency. It’s important to note that patient numbers in PEI are smaller, especially in the urgent triage category for psychiatry, so a longer wait for just a few can push reported numbers up.
Ill effects
Some experts say illness can get progressively worse the longer someone sits waiting. That creates the perverse situation whereby someone with relatively mild illness, who might benefit from quick intervention to prevent it from getting worse, will wait longer simply because they are not sick enough, yet.
“All of our systems triage based on urgency,” said Todd Leader, who now teaches part time at St. Mary’s University but until recently worked to overhaul the way mental health care was offered in the old South Shore Health Authority in Nova Scotia. “Those people, because of the triaging, will be put way down on the list and their wait time will be much higher.”
This leads to both patients, and doctors, exaggerating symptoms, just as Josh Lewis did when he showed up at the emergency at the Queen Elizabeth Hospital.
“I had a number of doctors tell me they put ‘suicidal’ down on a reference” Leader said.“It gets attention.”

caption
Todd LeaderDr. Julie MacDonald, director of mental health and addictions in the eastern zone of the Nova Scotia Health Authority, the area that includes the Cape Breton Regional Hospital, said one reason for the long waits is increasing demand.
“As we’ve worked in many communities to reduce stigma we have more people accessing services,” she said, “making it difficult to meet all the need.”
Not everyone agrees waiting lists necessarily cause illness to worsen.
David Zitner, a longtime family doctor and retired professor in the medical school at Dalhousie University, argues that there is actually little research to back up the contention that people who sit on waiting lists get sicker. “So unless you compare the rate of improvement of people on the waiting list with the rate of improvement for people who are sick, we don’t know whether the waiting period is helpful or awful.”
Last fall, controversy broke out when the Nova Scotia Health Authority wrote to people on the mental health waiting list in Cumberland County to ask if they had recovered on their own, and if their appointments could be cancelled. The authority later apologized, but the controversy underlines one of the problems with waiting lists, that no matter how considered a triaging process is, it is difficult for the system to know how sick somebody who is waiting really is, whether they have worsened, or even improved.
Shortages of professionals
One of the drivers of waiting times is a shortage of key mental health professionals. With numbers of psychiatrists and other clinicians lower in areas away from Halifax, one or two people leaving can cause a sudden jump in wait times.
Working in a smaller community may mean more time on call and no backup network of specialists to help with complex cases. This makes recruiting and retaining staff difficult, according to Dr. Ian Slayter, a psychiatrist in Antigonish who himself is on call at St. Martha’s Regional Hospital. His waiting list in his practice is six to seven months long he said, and the area has been working for almost a year to replace another psychiatrist who left.
While a replacement is coming, from Ireland, the red tape and immigration approvals mean the new doctor won’t be in place until the summer.

caption
Dr. Ian Slayer“Something that troubles me is that we don’t train enough psychiatrists for the province – or at least, we don’t train in a way that encourages them to stay in the province and (be) comfortable going out into small areas,” Slayter said. Of eight psychiatric residents who graduated from Dalhousie University’s medical school last year, he said, only one chose to practice in rural Nova Scotia.
Indeed, of the 169 psychiatrists listed as practicing in Nova Scotia, 113, or two thirds, list their practice location within Halifax Regional Municipality, or about three per 10,000 people. The remaining 56 are spread across the rest of the province. That’s about one per 10,000 people.
In PEI, there are 18 psychiatrists, 15 of whom work in Charlottetown and three in Summerside, about 1.2 per 10,000.
D’Orsay, who has been navigating the mental health system for years, says the revolving door of professionals is hard on patients.
“So you’re stuck back in a cycle of finding somebody again, building a relationship and a rapport with them, and then they’re gone and you’re back to square one,” she said. “So it can actually make you feel… that you’re not worth good quality care. And that you are the problem, and you are a burden, and I think that exacerbates mental health issues.”
For those with private medical insurance, or sufficient means, there is the option of seeking private care from psychologists or counsellors who charge by the hour. This can cut wait times, or allow people to get treatments otherwise unavailable. But there are shortages of those professionals too.
“Here in rural areas, it’s not uncommon to have psychologist positions go vacant for years,” said Shelley Goodwin, a psychologist practicing in Yarmouth, and president of the Association of Psychologists of Nova Scotia.
One rural Nova Scotia psychologist interviewed by King’s students, who asked we not use their name, said their own waiting list was two years long.
Which all reverberates back down to the level of people trying to access the care they need.
Sarah Stewart-Clark heard so many stories about the state of mental health services on PEI that she wrote to the premier, Wade MacLauchlan.
Stewart-Clark was co founder of the group Island Mothers Helping Mothers. It was initially set up as a way for mothers to share advice, and to provide financial and emotional support to one another. But soon, she was overwhelmed with stories about the mental health system.
“I’m absolutely stunned at the lack of care,” she said.
“They have this hotline, …they have some mental health walk-in clinics, and so it looks like there’s all these access points to make it easy for people to access the system. But calling any of those numbers, or visiting any of those walk-in clinics, essentially just puts you on the same wait list as everyone else.
“…The bottom line is there’s not enough specialists to deal with the number of people who need them,” Stewart-Clark said.
And also not enough family doctors.
Doctor shortage
For one Cape Breton woman, that’s made it tough to get care she needs.
The woman, who asked not to be identified due to her public profile, sat on a mental health waiting list for two years before getting a call at nine on a Saturday morning for a cancellation that had come up at 10. With her daughter and niece in her care, she couldn’t make the sudden appointment, “and I haven’t got another call since.”
To make things worse, she recently lost her family doctor.
“So for me to get my prescription filled, I’m going to have to go in and explain to somebody new who doesn’t know me why I have a yearly prescription to Xanax (an anxiety medication). So you know, it’s kind of right now there’s limited and next to no real resources I can use for my health issues.”
According to the Nova Scotia Health Authority, there were almost 28,000 people registered as searching for a family doctor in the province, as of April 26, more than 15,000 of them outside of Halifax and West Hants. A similar registry in Prince Edward Island listed almost 7,000 people in February.
Those numbers probably understate the real picture, because people have to actively register to be counted. In 2014, Statistics Canada reported that about 100,000 Nova Scotians were without a regular family doctor, and about 13,000 Islanders.
Family doctors not only provide basic front-line care, but their contacts and expertise can be the key to getting access to care in the formal mental health system.
Dr. Cathy Felderhof runs a family practice in Canso and at the Pictou Landing First Nation in northern Nova Scotia. She says she is usually able to get the mental health care she needs for her patients, but she credits her experience and contacts with making that possible.
“When someone doesn’t have a family doctor, they don’t have an advocate,” she said. “To understand the system and to navigate through the system, sometimes takes years of experience.”
Felderhof calls the number of people without a family doctor “astonishing.”
While it is true that in both Nova Scotia and PEI, people can also refer themselves to the mental health system, by calling a telephone number, without a family doctor overseeing your health, you may not even realize you are sick and need help.
“So a lot of my job, I’d say (for) a third to 40 per cent of people I see, depression and mental health issues are a significant player in what they present with,” said Dr. David Stewart of Cornwall, a suburb of Charlottetown. “Oftentimes I find myself in a position of almost having to sell them of the idea, or to convince them, that what they’re suffering from is in fact a mental health issue.”

caption
Dr. David StewartNova Scotia has been trying to manage the doctor shortage by supplementing physicians with other less-highly-trained and less expensive practitioners. As well, the Liberals’ April 27 budget, which died when the house was dissolved for the May 30 election, promised $2.4 million to recruit about 20 new doctors. Half of the money would go towards funding 10 more spots in the Dalhousie family medicine program, which has about a 75 per cent retention rate. The day before the budget, the CEO of Doctors Nova Scotia told the legislature the province needed at least 100 more doctors this year “just to break even.”
Not surprisingly, the issue already figures in the election campaign.
The Nova Scotia Conservatives are promising $13.5 million for a recruitment program to attract more doctors to areas most needing them, and a doubling of a tuition relief program that allows doctors to cut their student loan debt in exchange for moving to a rural area. The party figures these measures can add 50 doctors a year over the next four years, some of whom would be specialists such as psychiatrists.
The NDP has promised $30 million a year over four years to improve primary care and address doctor shortages, though is not promising a specific number of doctors.
More gaps
And there are yet more gaps in mental health services.
In PEI, a 10-year mental health and addiction strategy, released in late 2016, highlighted some of the missing pieces there. There is no adult day treatment programs of the kind found in Nova Scotia. In a day treatment program, people needing more intensive care spend their days at a hospital or community facility, and go home at night.
In Nova Scotia, some key supports for people that exist in the Halifax area, are not only non-existent in areas beyond Halifax, but in some cases, people from outside Halifax can’t access them.
And in both provinces, there is no equivalent of the mobile crisis team that operates in the Halifax area, bringing together a police officer and mental health workers to respond to people’s homes when they are in crisis. People outside these areas can call a crisis phone line instead.
Another huge gap is mental health care for the elderly. Jeanne Ferguson sees the evidence of this every day in her geriatric psychiatric practice in Boularderie East, half an hour’s drive northeast of Sydney.
While theoretically she can send ageing patients to the only specialized psychiatric inpatient unit for the elderly in Nova Scotia, called Willow Hall, at the Nova Scotia Hospital in Dartmouth, Ferguson says in practice it is nearly impossible to get a bed there. There’s just too much demand.
“In Cape Breton we have nothing so…our seniors who have mental health needs have to go to (regular) acute psychiatric beds, of which they are at a huge premium right now because they’re just aren’t enough of them. So it’s very difficult and…they’re not set up for the demented elderly,” she said.
“So that’s a huge stress on the system… (and) …we have folks who would probably benefit from a residential stay in a facility for the demented elderly who are in our nursing homes and we’re trying to manage them with sitters and security guards.”
The problem is greater in Cape Breton because the proportion of seniors in the population is higher than in comparatively youthful Halifax. “The numbers are huge,” Ferguson said.
Emergency in the emergency
The cumulative result of the lack of resources in a lot of communities is that people go to the emergency department and seek help there. Sometimes they sit for hours, see a mental health worker, and then are sent home or referred to a mental health service.
Numbers provided to King’s students through freedom of information show that from 2012 to 2016, 53,235 people, about 10,647 a year on average, were recorded as arriving at Nova Scotia Health Authority emergency departments with mental health as the presenting complaint. Of those, 31,121, or about 6,224 a year, visited emergencies in the three provincial health zones outside of Halifax and West Hants.
But the numbers almost may understate the extent of rural use because the reason for emergency department visits frequently goes unrecorded in areas outside Halifax, most notably at the Cape Breton Regional Hospital where the reason for two thirds of visits went unrecorded. By contrast, in Halifax, fewer than 10 out of 748,000 visits lacked a recorded reason.
“We’re sitting back, knowingly allowing people to get sick,” said Todd Leader. “And then where do they end up? …Instead of in an outpatient appointment where they should be, they end up in the emergency department.”
Courey believes the reasons for the use of emergencies may be somewhat complex. For example, she said it’s known that some people, especially young people, avoid treatment for mental illnesses due to stigma, then worsen and end up at emergency departments.
In Prince Edward Island, use of emergency departments for mental health concerns has slipped since 2012 though it increased slightly in 2016 at the two large, 24-hour facilities at the Prince County Hospital and the QEH, according to figures provided by Health PEI.
At roughly 25 emergency department visits per 100,000 people in 2016, this is still well above the numbers recorded in Nova Scotia.
Elaine Garland is one of the founders of the Pictou County Family Support Association, a volunteer group that helps people living with mental illness.
“So in the Aberdeen (Hospital in New Glasgow), you sit with your loved one who is of course having a breakdown and they can’t sit still. They pace and they might get loud and there could be a guy with a three-year-old child with the flu beside you,” she said. And so there’s no space where you can put someone in a calm room.”

caption
A waiting room at the Aberdeen HospitalKing’s students made several attempts to speak to emergency room doctors and others who work inside the emergency departments. Most declined, but one health worker from eastern Nova Scotia did talk about what happens when a patient in a psychiatric crisis arrives at the emergency department. The worker asked to remain anonymous as they were not authorized to discuss such matters publicly.
“(Patients) have to be medically cleared first, so they have to go through the process that everybody else in the emergency does where they are triaged. (Then) they wait however long, like a couple of hours for their turn, they see a medical doctor.”
Only after that, the worker said, does a patient go on to see a mental health professional.
“It would just be nice if there were an emergency mental health system, because (now) it just puts them in queue with everybody else that is waiting out in the waiting room…I feel that it is a different kind of care that they need and it is not getting taken care of in a timely manner there and people get frustrated.”
Tim Houston, a Conservative MLA up for for re-election in Pictou East, is blunter in his assessment.
“The way the system is kind of set up at the moment is that if a person feels like they are going to harm themselves or they are going to harm others they are supposed to report to the emergency room at the hospital… I find it inhumane to require people to get to that point.”
It’s also expensive to rely on hospital emergency departments for front line mental health care, said Dr. Chiachen Cheng of the Centre for Applied Health Research in Thunder Bay, Ontario. “If you think about a bed day you’re talking about a $1,000 a day,” she said.
Beds for the most critically ill
Province-wide in Nova Scotia, about four of five people who come to a hospital emergency department with a mental health complaint are seen and then sent home, sometimes with a referral to community-based services, and one in five is admitted to the hospital, according to a King’s analysis of figures provided by the Nova Scotia Health Authority.
Outside of Halifax Regional Municipality, that admission rate is typically much lower at hospitals that don’t have dedicated mental health beds, the analysis shows, and experts agree that acute beds are a critical part of the system.
While there is disagreement on the point, some feel there just aren’t enough of them.
In 2012, an expert report cautioned that Nova Scotia was already operating with a minimal number. The Come Together report was a massive review and blueprint for mental health services conducted by a group of 14 stakeholders from across the system. It found numerous problems with access to the care, long wait times, difficulty in navigating the system, and disparities of services across the province.
“The consequence of a shortage of beds, especially when combined with inadequate supportive housing and community supports, include: increased homelessness, the incarceration of mentally ill individuals, overburdened emergency departments, and increased violent crime,” the report said.
Come Together calculated that there were about 20 acute psychiatric beds for every 100,000 people, “low compared to other jurisdictions.” While it said the beds should be consolidated in fewer, larger locations, it said the number must not be reduced.
In late 2015, the Nova Scotia Health Authority closed the eight-bed, short-stay mental health unit at the Aberdeen Regional Hospital in New Glasgow, citing personnel shortages.
It was meant to be temporary, but the authority has never reopened it. Courey said a final decision on its future has not yet been made but in the meantime the authority has set up a “rapid access” service that allows for quicker and more intensive follow up for those visiting the emergency department.
The closest psychiatric beds are now in Antigonish, almost 60 kilometres to the east, and Truro, about the same distance to the southwest, and Courey said patients needing inpatient care are transferred to those hospitals when possible. Since the closure, 50 patients who would have otherwise been admitted to the Aberdeen have been transferred, 22 to Truro, 13 to Kentville, four to Antigonish, and the rest to a variety of locations, including one who was transferred to Yarmouth, figures provided by the Nova Scotia Health Authority show.

caption
Saint Martha’s Regional Hospital in AntigonishHouston said he has been hearing a lot of stories of officials scrambling to find patients a bed, only to find out there is nothing available.
“What’s happening now is people aren’t even bothering going into the hospital because they feel they are not going to do anything, so ‘”I’m not going to go right?’”
There are now 99 acute psychiatric beds in areas outside of Halifax Regional Municipality, according to information released by the Nova Scotia Health Authority through freedom of information.
That’s about the same 20 beds per 100,000 people that the Come Together report characterized as minimal five years ago. Including all of the specialized psychiatric beds at the Nova Scotia Hospital and the QEII, there are about 25 beds per 100,000 province-wide under the Nova Scotia Health Authority.
Courey said the authority has studied bed utilization, and she doesn’t think any more beds are needed outside Halifax.
“It’s important that you have them and you use them when you need them, but they are by no means, in and of themselves, an adequate treatment modality for the vast majority of people with mental health disorders.”
She said one problem that does exist is that beds, especially in the central zone, are often occupied by people with complex problems who ought to be moved into some other kind of facility, but can’t be because there is no room.
In PEI, there are actually a lot more acute psychiatric beds per capita than in Nova Scotia, with about two thirds at the Hillsborough Hospital. There are 24 at the QEH, and there, the system strains against capacity.
“At busy times, there are about 10 people waiting in the emergency room for a bed,” said long time Island psychiatrist Dr. Benjamin Spears. “You can’t admit everyone who is talking suicide – there aren’t enough beds. You have to make sure they have the capacity to come back if they get worse or contact someone. It raises the stakes and it makes work much more stressful. I think you get more burnout in the system with less beds.”
Until 2014, Dr. Margaret Kennedy was the director of mental health and addictions in PEI. She said managing the beds is a challenge, and patients do end up waiting in emergency, but doctors try to manage it.
“There’s a lot of work going on in a lot of different places to determine how can we make a bed available to that person who needs it, and in the meantime, provide them safe care.”
People feel let down
All of this, shortages of professionals, limited beds, limited community programming compared to Halifax, and a reliance on emergency departments to handle crises, leaves some patients King’s students spoke to feeling the system lets them down.
Twyla Wilband has become a sophisticated consumer of mental health services, due to her many years of accessing the system.
Wilband grew up in New Brunswick, but moved to Truro when she was 16. She has had many different treatments over the years.
When her long-time therapist went on sick leave, “she was basically burnt out, so to speak, there were no services, no one seemed to pick up any of her clients, so all of her case load dropped.”
Now, Wilband she says she’s being told the only option for her is group therapy, even though she doesn’t feel it’s right for her.
“I’ve lived this journey, I know what I need and what I don’t need, and they’re not willing to work with somebody that knows what they need.”
Cecilia McRae, a retired schoolteacher and past president of the Schizophrenia Society of Nova Scotia, contends the system has the wrong priorities.
“This is not just something that’s happening in Pictou County only; it’s pretty well right across the province and right across Canada, where the people themselves are not the focus of the health care,” she said. “The system itself has become more important than the person.”

caption
Pictou CountyPatients are told, “‘this is what we have, and this is what we’re going to give you whether you need it or not, and whether its appropriate or not.’”
Some go so far as to say the entire system is in crisis.
“It was just shocking to me, and I felt that if I didn’t start speaking out against it, that I was complicit in living in a community where we treated the most vulnerable in the way that we were treating them,” said Stewart-Clark of Island Mothers Helping Mothers.
She recently took her concerns to the Island’s health minister.
Robert Henderson acknowledges there are many challenges.
“It’s just a really complex issue, the whole subject of mental health, and I don’t know if there is any one jurisdiction we could point to that you could say, ‘that jurisdiction has got it down right,’ he said.
“We’re just trying to find our way just like an other jurisdiction.”
PEI has made a number of recent changes, announcing $600,000 in security upgrades at the Hillsborough Hospital, three new walk-in mental health clinics in Prince County, and a new program to put mental health nurses into schools.
Henderson says with PEI’s small population, and equally small pools of specialists, even the loss of one psychiatrist going on maternity leave or moving away, can have a big impact. He says there is a lot of competition to hire such professionals, and at the same time, more and more people are seeking services, both because of lowered stigma and changes in society.
“We feel we have lots of services in place, help lines, lots of supports that are out there that we are implementing,” he said, “but is it ever enough and does it meet a crisis situation? Sometimes it doesn’t, and as much as we can regret that, we’ll try to do the best we can to accommodate people in need.”
Stewart-Clark believes there is still a long way to go.
“I wrote a letter to Premier MacLauchlan to describe what I saw after dealing with these families for three years. And in between sending that letter, and hearing from him, we had three suicides of young people in their 30s, and two of them were mothers in our group. And I just thought, I can’t wait any longer to try to alert the province to this issue.”
Across Northumberland Strait, on Nov 1, 2015, Nova Scotia Opposition Leader Jamie Baillie introduced a private member’s bill in the provincial legislature to call a public inquiry into mental health in the province. The party followed up with an emergency debate on mental health care at Province House, but the Health Minister Leo Glavine rejected any suggestion of a crisis. Instead, he assembled a panel of experts to make recommendations.
That panel, which included Todd Leader, made four recommendations, largely focused on youth mental health and programs in schools, and also proposed a province-wide web and telephone service, answered 24 hours a day, to provide more consistent access to mental health services across the province. The government promised to implement all of the recommendations.
Despite this, and despite the health authority’s long-term plan to improve services, Baillie, now campaigning to be premier, maintains the system is in crisis.
“We can’t go on like this,” he said. “We need a very active government to put in place supports for families who are facing mental illness.”
But Courey says not only is there no crisis, but with the new authority, there is an opportunity to create a system to be proud of.
“I guess you’ll wait to see over the next few years, as we try to show that the advantage of the creation of the NHSA, the advantage of sound planning based on evidence, and then we’ll show ya,” she said. “What you see often is people talk about the system being in crisis when they or their loved ones couldn’t access they service they felt they needed.”
Courey fears that even calling it a crisis can undermine the credibility of the system, and discourage people, especially young people from seeking care.
“There are many hundreds and thousands of people who are being helped by our clinicians and psychiatrists every day,” she said.
“Cycling uphill”
Dr. Michael Teehan, the head of psychiatry at Dalhousie, says one of the reasons change is difficult is that mental health has to compete with physical health care for scarce government resources.
“At every level – the national level, the provincial budget level, and within hospitals – it is invariably difficult to compete with the acute services for which you can claim that unless something is done, patients will die,” he said. “Patients die of their mental health disorders, but they do it more slowly, less publicly, and less demonstratively for this kind of pressure to be put on.”
Dr. Spears, who began his long Island career in psychiatry after immigrating from England, agrees mental health has still not really broken away from the stigma and prejudice that have always afflicted it.
“So people working in mental health are always, in one sense, cycling uphill. There’s no level ground, and that’s a fact of existence,” he said.
“In the twilight of my career, that’s the conclusion I’ve come to.”

